A Primer On Cardiac Auscultation
Robert T. Herrington, M.D.
Copyright © 1980, Robert T. Herrington
The following discussion presents a method of understanding the anatomical and physiological basis for auscultatory findings in various cardiac abnormalities. This method has been used for a number of years in a lecture-demonstration course given to medical students and
requests have often been made that it be "written up". The discussion is not a detailed treatise on auscultation; rather it is hoped that the concepts presented will establish a framework upon which the beginning student might develop further the exciting skill of cardiac auscultation.
In order to understand where on the anterior chest to listen for the noise which occurs with various cardiac lesions, it is necessary to appreciate fully the anatomy of the heart and
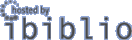
the great vessels in relation to the precordium. A model of the two ventricles and the great vessels can be formed with your hands. As shown in Figure 1, the right hand so folded and held
in space represents the left ventricle from which comes the aorta. Also, this hand model is actually a fair representation of the muscular configuration of the left ventricle-an elliptical structure whose musculature is ideally arranged for pressure pumping.

Figure 1
A hand model of the left ventricle with the index and middle finger representing the aorta. The palm of the hand represents the interventricular septum or septal surface of the right ventricle. The thumb may be considered to be the Crista supraventricularis-above the thumb the outflow portion of the right ventricle and below the thumb the inflow portion of the right ventricle.
The left hand, as shown in Figure 2, represents the right ventricle. Here again the left hand so arranged represents & fairly accurate functional model of the right ventricle--a billows type or volume pump. Interestingly, the way that the thumb and fourth and fifth finger of the right hand are held depicts a reasonable model of the septal surface of the right ventricle. The area above the thumb represents the outflow portion of the right ventricle; the thumb represents the crista supraventricularis; and the area below the thumb represents the inflow portion of the right ventricle.
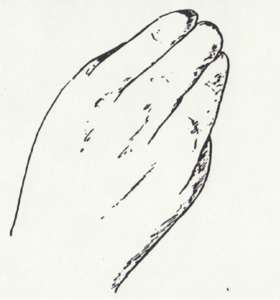
Figure 2
A hand model of the right ventricle.
With the two-handed model (Figure 3), it is seen that the left ventricle lies postero-inferior and slightly to the left of the antero-superior and rightwardly placed right ventricle. From an antero-posterior projection only a relatively small portion of the left ventricle is visible.
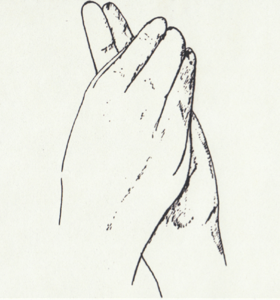
Figure 3
A hand model of the heart. The right hand represents the left ventricle and the ascending aorta and the left hand represents the right ventricle and origin of the pulmonary artery.
The index and middle fingers of the right hand represent the aorta originating from the left ventricle which is behind the right ventricle. One can project its course as it passes antero-superiorly and to the right in order to give off the brachiocephalic vessels as it forms an arch and descends posteriorly on the left side of the vertebral column. The ends of the index, third, and fourth fingers of the left hand represent the outflow portion of the right ventricle and the beginning of the pulmonary artery. The pulmonary artery courses posteriorly and divides into the right and left pulmonary arteries.
The atrial relationships to the ventricles can also be approximated by use of the hands. By cupping the left hand behind the left ventricular model, the left atrium can be represented. By cupping the right hand to the side of the right ventricular model, the right atrium can be represented. For the purpose of this discussion, however, it is not necessary to depict these structures in our model because the atria are not in immediate contact with the anterior chest wall.
If the heart model is now placed into the anterior mediastinum as shown in Figure 4, it is apparent immediately that areas can be localized on the precordium to which a stethoscope might be placed in order to be nearest to either of the outflow portion of the right ventricle and the beginning of the
pulmonary artery. The pulmonary artery courses posteriorly and divides into the right and left pulmonary arteries.
The atrial relationships to the ventricles can also be approximated by use of the hands. By cupping the left hand behind the left ventricular model, the left atrium can be represented. By cupping the right hand to the side of the right ventricular model, the right atrium can be represented. For the
purpose of this discussion, however, it is not necessary to depict these structures in our model because the atria are not in immediate contact with the anterior chest wall.
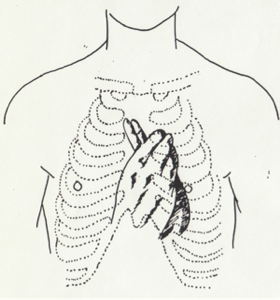
Figure 4
A hand model of the heart. The right hand represents the left ventricle and the ascending aorta and the left hand represents the right ventricle and origin of the pulmonary artery.
If the heart model is now placed into the anterior mediastinum as shown in Figure 4, it is apparent immediately that areas can be localized on the precordium to which a stethoscope might be placed in order to be nearest to either of the ventricles or great vessels. Although somewhat more distant
from the anterior chest wall than the other three structures, the second right intercostal space (upper right sternal border) is where the stethoscope is as close as it can get to the proximal aorta. At the second left intercostal space (upper left sternal border) the stethoscope is placed very close to the pulmonary artery. At the third and fourth left intercostal spaces (lower left sternal border) it is over the right ventricle. Finally, at the apex (fourth and fifth left intercostal space in the midclavicular line) it is closest to left ventricle.
With this understanding of the anatomy of the heart and its relation to the anterior chest wall, four areas may be localized - aorta, pulmonary artery, right ventricle and left ventricle. In textbooks on physical diagnosis, these four locations are given the names "aortic," "pulmonary," "tricuspid," and "mitral" valve areas. Obviously this is a misconception. Noises that are heard with lesions of the respective valves are heard at those areas, but, as will be developed below, the noises are occurring actually in the aorta, pulmonary artery, right ventricle and left ventricle or structures attached to them.
This leads to the next obvious but important concept regarding auscultation. That is, a noise occurring in a structure of the heart has a tendency to be transmitted to attached structures. For instance, a noise that is actually occurring in the left atrium-a structure which is very deep within the chest and to which a stethoscope cannot be closely placed, will be transmitted and heard best over the left ventricle. It might also be expected to be heard well in the left axilla. Similarly, noises occurring in the right atrium, which is somewhat closer to the chest wall than the left atrium but still not in immediate contact, will be transmitted to and heard best when listening over the right ventricle. The same reasoning holds for a noise in the aorta. Not only will it be heard well at the upper right sternal border, but might be expected to transmit diagonally across the precordium to be heard in the left ventricle or at the apex. Pulmonary artery noise will be transmitted not only to the back but also to the right ventricle, and will have a vertical distribution along the left sternal border.
It is appropriate now to begin a discussion of the origin of noise that might occur with various cardiac lesions. At this point, the noise under consideration will be murmurs. A murmur will occur whenever there is turbulence with enough energy to be audible, and turbulence will occur in the chambers of the heart and in the great vessels under the following conditions:
(1) When there is an abnormal connection between two structures that have a significant pressure difference at a time in the cardiac cycle.
(2) When there is increased flow through either normal or abnormal structures.
(3) When there is an abnormal pressure difference between two structures during a phase in the cardiac cycle.
Condition 1: An abnormal connection at times of significant pressure difference may be stated simply as a "leak". The expanded definition is purposely used, however, because one must know the pressures in each of the structures during the phases of the cardiac cycle. These normal pressures are shown in Figure 5. By using this information, one may easily deduce where and when a leak might occur. The turbulence produced will be located in the structure into which the leak is occurring, i.e. the structure with the lower pressure.
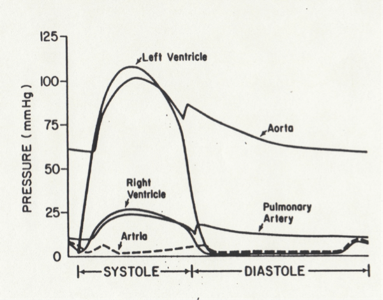
Figure 5
A representation of the pressures in the various chambers of the heart and great vessels during the cardiac cycle. For simplicity the atrial pressures are considered to be equal.
Condition 2: A pressure difference which ordinarily would not be present may be simply defined as an “obstruction". When this condition is present the pressure will be elevated abnormally in the structure proximal to the obstruction. It is seen in Figure 5 that there is no significant pressure difference normally between the ventricles and their respective great vessels during systole or between atria and their ventricles during diastole. However, if there is ventricular outflow obstruction the ventricular pressure will be elevated; if there is atrioventricular obstruction the atrial pressure will be elevated. When Condition 2 is present the turbulence produced will be located in the structure distal to the obstruction.
Condition 3 The turbulence produced by increased flow will be located in the structure into which the increased volume of blood is being pumped. One might think of this condition as being a "physiologic obstruction".
Using the information presented to this point, one should be able to reason where on the anterior chest wall and when during the cardiac cycle the murmurs of various cardiac lesions can be heard. To demonstrate let us apply Condition 1 to lesions of the left side of the heart.
There is normally a pressure difference between the left ventricle and the left atrium during systole (as seen in Figure 5); thus mitral insufficiency would satisfy this condition. Such a "leak" would produce turbulence in the left atrium during systole. From our understanding of anatomy and the transmission of sounds, it would be reasonable to assume the noise could be heard over the left ventricle; therefore, the murmur of mitral insufficiency is a systolic murmur heard best at the apex because that is where the stethoscope can be placed the closest to the left ventricle. The murmur might also be heard well in the axilla because the noise will be transmitted to the
left lung.
Another left-sided lesion satisfying Condition 1 would be a ventricular septal defect. Referring again to Figure 5, one notes that a pressure difference occurs between the right and left ventricles during systole; hence a "leak" between the two ventricles would cause turbulence which would be in the right ventricle and the murmur would be best heard at the lower-mid left sternal border. Likewise, there normally exists a pressure difference between the aorta and the left ventricle during diastole. If there is a lesion of aortic insufficiency, there would be a "leak" occurring into the left ventricle during diastole resulting in a murmur heard in the left ventricle and transmitted to the aorta. Thus, the murmur of aortic insufficiency is a diastolic murmur heard diagonally from the upper right sternal border to the apex.
The final lesion on the left side to be considered is an abnormal connection between the aorta and the pulmonary artery--or a patent ductus arteriosus. It is seen from Figure 5 that there is a pressure difference between the aorta and the pulmonary artery throughout the cardiac cycle. The leak would be into the pulmonary artery and would be continuous throughout the cardiac cycle. Therefore, it can be deduced that the murmur of a patent ductus arteriosus would be a continuous murmur heard best at the upper left sternal border where the stethoscope is placed closest to the pulmonary artery.
Using the same reasoning, one realizes that murmurs of right--sided lesions fitting Condition 1 would be tricuspid insufficiency which produces a systolic murmur heard best at the lower left sternal border and pulmonary insufficiency which produces a diastolic murmur heard best along the left sternal border.
Applying Condition 2, obstruction, one observes that left-sided murmurs might occur because of mitral stenosis or aortic stenosis. With mitral stenosis, there would be an abnormally elevated left atrial pressure in relation to left ventricular pressure during diastole; therefore, as previously discussed, there would be turbulence in the left ventricle in diastole and the murmur of mitral stenosis should be heard best at the apex in diastole. With aortic stenosis, there would be an abnormally elevated left ventricular pressure in relation to aortic pressure during systole. Turbulence would be occurring in systole in the aorta; thus the murmur of aortic stenosis is reasonably assumed to be a systolic murmur which would be heard best at the upper right sternal border. It would also be expected to radiate diagonally across the precordium to the apex. Right sided lesions would be tricuspid stenosis and pulmonary stenosis. The former would cause turbulence in the right ventricle and would be heard best at the lower left sternal border. Pulmonary stenosis would cause turbulence in the pulmonary artery and would be best heard at the upper left sternal border.
A number of Important murmurs have their origin based on the third condition for turbulence, an increased flow through structures or a "physiologic obstruction”. Fever, anemia, pregnancy, and thyrotoxicosis all cause an increased cardiac output. As the semilunar valve rings are smaller than the atrioventricular valve rings, the turbulence associated with those conditions would be greater in the pulmonary artery and aorta. Because the stethoscope can be placed closer to the pulmonary artery than the aorta, one can thus assume that the murmur of pregnancy, anemia, etc. would be in systole and best heard at the upper left sternal border. This does not preclude the possibility that such a murmur may be heard over the aorta.
The murmurs of an atrial septal defect also occur as the result of an increased volume of blood being pumped through normal structures. With an atrial septal defect the atria may be considered a common reservoir. Because the right ventricular compliance is greater than the left, there is preferential filling of the right ventricle during diastole. This increased right ventricular volume being pumped into the pulmonary artery during the next systole will produce turbulence in that structure. Therefore, the murmur of an atrial septal defect will be a systolic murmur heard best at the upper left sternal border. There is also the possibility of having turbulence in the right ventricle early in diastole as the right ventricle is being presented with the increased volume of blood.
Early diastolic turbulence in the left ventricle produces a very important murmur with which to be familiar. This murmur can be caused by an increased volume of blood being presented to the left ventricle. With a ventricular septal defect or a patent ductus arteriosus, there is increased blood flow
through the lungs that results in a greater volume being presented to the left ventricle during diastole. A similar situation is present with mitral insufficiency as the retrograde flow resulting from the leak during systole is added to that coming from the lungs and then is presented on the next diastole to the left ventricle. This diastolic murmur in the left ventricle is valuable as it allows a certain quantification of the amount of shunting that is occurring as the result of a ventricular septal defect or patent ductus arteriosus, as well as the volume of regurgitation that occurs with mitral insufficiency. Interestingly, this logic allows one to understand that the hemodynamic abnormality of a ventricular septal defect is principally a volume load on the left ventricle rather than the right ventricle.
The discussion to this point has provided an approach to thinking about how a murmur can result from a variety of lesions. It has not addressed the subject of discerning the specific lesion associated with a given murmur. An analysis of heart sounds is helpful for this purpose.
A great deal of physiologic information may be obtained from an analysis of the timing of the two components of the second heart sound. In the normal second heart sound, the aortic component precedes the pulmonary component, and they move in relationship to each other during the respiratory cycle. There are two reasons for aortic closure preceding pulmonary closure. The pressure in the aorta is much greater than the pressure in the pulmonary artery, thus the aortic valve is closed more rapidly. This idea may also be understood in terms of compliance. As compliance of the pulmonary circulation is so much greater than that of the systemic, the pulmonary valve can "hang open" longer than the aortic valve.
The second reason for early aortic valve closure results from the anatomic arrangement of the conduction system. The bundle of His divides early into the right and left bundles. The left bundle crosses the septum and ramifies within a short distance on the left side of the septum and left ventricle. The right bundle courses down the right side of the septum and proceeds a longer distance in the process of delivering stimulation to the right ventricle. Consequently the left ventricular contraction is initiated slightly before the right, therefore, it may complete its systole first. The fact that conduction does play a role in the timing of the components of the second heart sound will be given more consideration later in the discussion.
The movement of the two components of the second heart sound in relationship to each other is explained by the fact that during the respiratory cycle there is a variable volume of blood presented to the right and left ventricles, and that the duration of the ventricular systole is directly related to the volume of blood which the ventricle must eject. During inspiration there is enhanced negative intrathoracic pressure which facilitates systemic venous return to the right side of the heart. At the same time the lungs are expanding, causing a decrease in the amount of blood being presented to the left side. This increased volume of blood coming to the right ventricle and decreased volume of blood returning to the left results in the right ventricle taking slightly longer to expel its ejection fraction and the left ventricle being able to accomplish it more quickly. Therefore, at the end of inspiration there is normally maximal splitting of the second heart sound. The physiologic principle is that the length of time that a semilunar valve stays open is related to the volume of blood that must be pumped through it.
A second physiological principle that plays a role in timing of the aortic and pulmonary valve closure is the resistance to outflow of blood from a ventricle. If it is more difficult than normal for a ventricle to eject its blood as would occur in aorta or pulmonary stenosis, it takes longer to do it.
In summary, there are three factors that play a significant role in the timing of closure of the semilunar valves--conduction, volume ejected through the valve, and resistance to ejection. One may apply these facts to explain what may be happening when the second heart sound is split on expiration rather than on inspiration. This would be the reverse of normal and is called paradoxical splitting. It may be the result of a delay in closure of the aortic valve to a point that it follows the pulmonary valve closure. In this case, when the right ventricle is presented during inspiration with an increased volume (and the left a decreased volume) the two sounds move closer to each other. The various possibilities that might lead to paradoxical splitting may now be considered: (1) Conduction. Obviously, left bundle branch block with a delay in activation of the left ventricle might allow aortic valve closure to be delayed beyond pulmonic valve closure. (2) Volume. An increased volume of blood which must be pumped into the aorta by the left ventricle would cause the aortic valve to stay open longer than normal. Aortic insufficiency would be an appropriate cause, but if that were the reason of the volume load the aortic valve might be so abnormal that its closure noise may not be heard. Another situation in which the left ventricle has an increased volume that must be pumped into the aorta is with a patent ductus arteriosus. With a left to right shunt into the pulmonary artery there is increased volume of blood traversing the lungs, thus increasing left ventricular volume. If this increased volume is large enough, it will require the aortic valve to stay open longer and cause paradoxical splitting. This is not a very useful physical finding because the murmur of the ductus would probably be so loud that the second heart sound might not be heard clearly. The important point, however, is the principle involved, and paradoxical splitting with a patent ductus arteriosus has been confirmed. In other situations in which there is a left ventricular volume load, i.e., mitral insufficiency and ventricular septal defect, the principle is not involved because the excess volume of blood pumped by the left ventricle does not traverse the aortic valve. (3) Pressure load. This may best be illustrated by aortic valve stenosis. If the obstruction is severe enough, left ventricular ejection time is delayed to the point that paradoxical splitting is heard and the possibility of severe stenosis is likely. Even close or difficult to hear splitting of the second heart sound with the murmur of aortic stenosis raises the possibility of significant obstruction.
Using the same principles one can understand why, in the presence of right bundle branch block or significant pulmonary valve stenosis, the second heart sound might be more prominently split than normal. However, the normal movement with respiration would be present because there would still be the previously described volume changes occurring in the right and left ventricles during respiration.
The presence of both components of the second heart sound is obviously an important consideration in the evaluation of congenital heart disease. If a semilunar valve is not present or the flow through it and the pressure distal to it are so low that the component cannot be audible, the second heart sound will be perceived as single. Such an auscultatory finding would be important in the consideration of such defects as tetralogy of Fallot, pulmonary atresia, tricuspid atresia, and hypoplastic left heart syndrome.
The quality of the sound that occurs at the time of semilunar valve closure provides useful physiologic information. If the pressure in the system distal to the valve is elevated one might expect that the noise associated with valve closure would be louder. In the evaluation of congenital heart disease, pulmonary arterial pressure is an important consideration and a loud pulmonary valve closure leads to the suspicion that pulmonary hypertension is present. In children, pulmonary closure is often relatively intense. An auscultatory trick involving the previously discussed principle of transmission of noises might help the listener decide if it is, in fact, abnormally loud. Because noises transmit to structures which are attached, it would be reasonable to hear splitting of the second heart sound when listening over the right ventricle or lower left sternal border, but not when listening over the left ventricle or apex. Therefore, if splitting of the second heart sound can clearly be heard when listening at the apex, it should raise the suspicion that the intensity of pulmonary closure is louder than normal and pulmonary hypertension is a possibility.
For a final discussion of the second heart sound and how the physiology of a cardiac defect might alter it, let us consider an atrial septal defect. It has already been pointed out that the hemodynamic abnormality of an atrial septal defect is a volume load on the right ventricle; therefore, it is expected that the pulmonary component of the second sound might be delayed. In addition, with an opening between the two atria the reciprocal difference in ventricular filling that occurs with respiration would not occur. Thus, there would be a constant volume of blood being presented to the right ventricle. The result would be prominent fixed splitting of the second heart sound. This abnormality of the second heart sound is characteristically present with an atrial septal defect.
A detailed analysis of the first heart sound is not necessary for this discussion. However a sound that is closely associated with the first heart sound is very useful in identifying systolic murmurs that are heard best in either the pulmonary artery or the aorta. The noise is called an ejection sound or click and may be perceived as a very prominent split to the first heard sound. The origin of the sound is attributed to the sudden cessation of movement which occurs when a stenotic semilunar valve has reached its point of maximum opening . The ejection sound associated with aortic valve stenosis has a tendency to be distributed diagonally across the precordlum and may often be heard at the apex. With pulmonary valve stenosis the ejection sound has a vertical distribution along the left sternal border and varies in intensity with respiration. If assessing a murmur that is distributed across the precordium from the aorta to left ventricle that is thought to be aortic stenosis but an ejection sound or click is not heard it would suggest subvalvular obstruction.
In a similar manner it might be assumed that a stenotic atrioventricular valve could make a noise when it reaches its point of maximum opening. In the case of mitral stenosis the sound is heard early in diastole over the left ventricle and is called an opening snap.
The following is an attempt to bring together the various principles that have been discussed to show how the analyses of murmurs and sounds might logically lead to an anatomical diagnosis.
Assume that when listening to a patient, a murmur is best heard at the upper left sternal border and occurs in systole. Anatomically it would be reasonable to assume that the noise was in the pulmonary artery. Applying the first condition for the cause of turbulence (an abnormal connection between two structures having at a given time in the cardiac cycle a significant pressure difference) one might consider a patent ductus arteriosus. However if that were the case, that murmur would be expected to continue throughout the cardiac cycle because normally there is always a difference between the aorta and the pulmonary artery. As the murmur under consideration was only heard in systole, a patent ductus arteriosus would not be an appropriate diagnosis. But, for the sake of completeness, how might the turbulence in pulmonary artery with a patent ductus arteriosus be affected if there were increased pulmonary vascular resistance? If that were the physiological situation the pulmonary artery diastolic pressure might approach the aortic diastolic pressure and there would not be enough turbulence occurring in diastole to be heard, thus the typical continuous murmur of a pulmonary ductus arteriosus would not be present. What might be listened for to rule out that possibility? If there were pulmonary hypertension, the pulmonary component of the second heart sound might be increased in intensity to the degree that it was heard where it should not be, that is, over the left ventricle. In the hypothetical case, splitting was not heard at the apex so it may be assumed that the pulmonary component was not unusually loud and that pulmonary hypertension was unlikely. So the diagnosis of patent ductus arterlosus with pulmonary vascular disease may be ruled out.
The second condition for turbulence (an abnormal gradient between structures at any given time in the cardiac cycle when there usually is not a significant pressure difference) could be the reason for the murmur. If that were the situation, pulmonary valve stenosis could be the diagnosis. When a stenotlc pulmonary valve reaches its point of maximum excursion, a noise called an ejection sound--which may be perceived as a prominent split of the first heart sound--might be heard. In the hypothetical case under consideration such a sound was not heard; therefore, the possibility of pulmonary valve stenosis will no longer be considered. If an ejection sound had been heard and pulmonary valve stenosis was thought to be the cause of the murmur, attention to the second heart sound would have been appropriate. If the obstruction were severe,
the ejection time of the right ventricle would be delayed and prominent splitting with normal movement might be perceived.
The third cause for turbulence (abnormal volume of blood being pumped through normal structures) might also be the reason why a murmur is heard in the pulmonary artery. The simplest anatomic situation causing this physiologic abnormality would be an atrial septal defect. To confirm that possibility, an analysis of the second heart sound would be necessary. If it was heard as prominently split without change in the splitting during respiration, this might be due to an increase in volume being pumped by the right ventricle and a lack of the reciprocal changes of ventricular filling with respiration. Both of these phenomena would occur with an atrial septal defect. Thus an appropriate diagnosis of the hypothetical case could be proposed. If such were the situation, careful auscultation over the right ventricle early in diastole might reveal a right ventricular diastolic filling murmur, in addition to the systolic murmur in the pulmonary artery.
Next consider a situation in which a murmur clearly is heard best at the lower left sternal border during systole. From our knowledge of anatomy, one might assume that the turbulence is occurring in the right ventricle or a structure in continuity with it, i.e., the right atrium. The only reason for such a murmur would be an abnormal connection. A ventricular septal defect or tricuspid insufficiency would be possibilities. What other murmur might be present resulting from the third condition that could allow definition of the cause of the systolic murmur in question? If tricuspid insufficiency were significant enough, it would be possible to have a murmur in early diastole in the right ventricle due to an increased volume of blood coming back into the right ventricle. If the right ventricular systolic murmur were due to a ventricular septal defect, it would be possible that the left to right shunt was great enough to hear a left ventricular diastolic filling murmur. If such an early diastolic murmur were heard over the left ventricle, one could confidently assume that the lower left sterna border systolic murmur was due to a ventricular septa! Defect and that there was a significant left to right shunt.
For a third hypothetical case, assume that a systolic noise is heard best at the upper right sternal border and also heard well diagonally across the precordium to the apex. This would strongly suggest that the noise was in the aorta and it would be most appropriate to consider the second condition causing turbulence--obstruction. The anatomical lesion would be aortic valve stenosis. To confirm this diagnosis one would listen for a prominent split of the first heart sound or what, in fact, might be an ejection sound. If this is present, the diagnosis of aortic valve stenosis is confirmed. What other information might be obtained from auscultation that could possibly identify the severity of obstruction? Close attention to the second heart sound would be helpful. If left ventricular ejection time were delayed by severe obstruction, the point of aortic closure might actually occur later than pulmonary closure and paradoxical splitting would be heard. However, in the discussion of factors that might cause an alteration in timing of components of the second heart sound, one will recall that abnormal electrical conduction might cause paradoxical splitting. To rule this out an electrocardiogram would be necessary.
An analysis of the specific characteristics of murmurs is not necessary for this discussion. There is, however, a very important murmur for which the cause remains obscure, therefore a description is necessary. This is the innocent vibratory murmur of childhood. The murmur is best heard over the right and left ventricle at the lower sternal border and toward the apex, and not infrequently transmits to both the pulmonary artery and the aorta. It is a short, early to mldsystolic noise that has a harmonic or pleasant quality. The murmur is very characteristic and is not mimicked by a pathological condition. On a purely speculative basis this writer considers the origin of the sound to be noise associated with the contraction of young healthy myocardium.
Finally, It might be useful to make a few suggestions that are important In practicing the art of auscultation. First of all it is obvious that a good stethoscope is necessary. Frequently, inexpensive stethoscopes do not have diaphragms that will allow soft, high frequency murmurs to be heard. Secondly, auscultation is not a practice that can be accomplished briefly. All of the anatomic areas need to be listened to carefully with both the diaphragm and the bell with repeated comparisons made of the sounds occurring at the respective anatomical regions. With practice, the auscultator can learn to focus on a particular phase of the cardiac cycle, thus damping out noises that might detract. Finally, in order to obtain the concentration that is needed to hear adequately, one must minimize distracting events. A quiet room and, in the case of children, a quiet child is necessary. Any sensory Input has the potential of detracting from the acuteness of that which is under consideration. For this reason, individuals will often close their eyes when listening intently. Proprioception is another form of sensory input that may be detracting. To hear well one must be comfortable. Leaning over a person who is in bed will not allow one to hear as well as sitting comfortably beside the patient. These are all minor but important points.
One of the exciting aspects of cardiology is how much anatomy and physiology may be understood from physical findings. In this presentation only a small amount of the
information that is available has been covered. That Is intentional as its purpose is not primarily to present facts but rather to present a method that allows one to understand the origin of the facts. Most of the material presented in the discussion is thoroughly covered by McKusick, Leathern and Craige and they should be referenced for further study.
Additional Reading
McKusick, V. A. Cardiovascular Sound In Health and Disease. Baltimore, Williams and Wilkins Co., 1958.
Leatham, A. Auscultation of the Heart and Phonocardiography. 2nd Ed. New York, Churchill Livingstone, 1975.
Craige, E. Chapter 3. Heart Sounds. Phonocardiography; Carotid, Apex, and Jugular Venous Pulse Tracing; and Systolic Time Intervals. Chapter 4. Echocardiography and Other Noninvasive Techniques to Elucidate Heart Murmurs and to Solve Diagnostic Problems, in Braunwald, E. (Ed.) Heart Disease. A Textbook of Cardiovascular Medicine. Philadelphia, W.B. Saunders & Co., 1980.